Too much Stress and Pressure
license.
Some people with amyotrophic lateral sclerosis or frontotemporal dementia accumulate deposits of the nuclear pro- tein FUS in the cytoplasm. What drives this relocation? Researchers led by Mag- dalini Polymenidou at the University of Zurich blame osmotic pressure.
UniProt is a bit vague when it comes to the RNA-binding protein FUS: “May play a role in maintenance of genomic integrity.” What is certain: In healthy cells, FUS is transport- ed to the nucleus and binds to both DNA and RNA, mediating the synthesis of a whole range of proteins. But in ALS and frontotem- poral dementia – a common dementia – the entry of FUS into the nucleus of nerve cells is compromised. Aggregates of FUS and RNA transform into so-called stress granules. The role of these granules in the pathological process is still unclear.
Frontotemporal dementia is the second most common type of dementia after Alzhei- mer’s disease and typically affects individuals under 65 years of age. In a subset of these patients, affected neurons present a charac- teristic pathology with cytoplasmic mislocal- ization and aggregation of the RNA-binding protein FUS, which normally resides in the nucleus. Since no mutations in FUS or any other proteins have been described in these cases, the trigger of FUS mislocalization that likely initiates the cascade of events leading to neuronal dysfunction and death remains enigmatic.
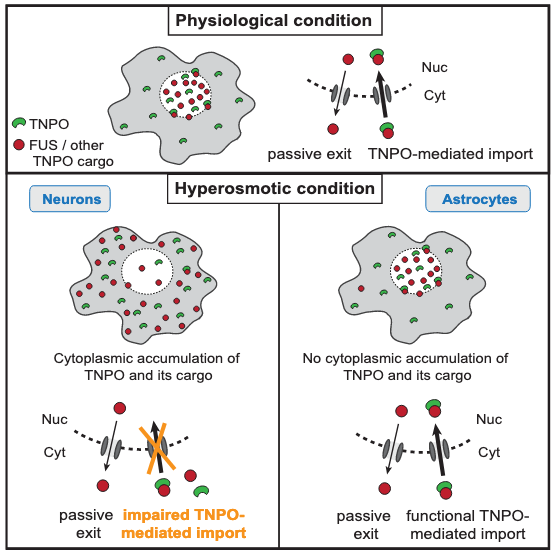
The new study by the Polymenidou group, published in Cell Reports, shows that hyper tonic stress leads to cytoplasmic translocation and loss-of-function of neuronal FUS. Surprisingly, and opposite to current thinking, the osmosis-triggered cytoplasmic shift of FUS is independent of stress granule formation or the molecular pathways induced by hyperosmolarity in cells.
FUS mislocalization could be the first step toward disease, Polymenidou suggested. She believes osmotic stress acts as the trigger that sends FUS to the wrong place, where a second stressor could then cause it to aggregate. An important implication of the work for public health is the fact that hyperosmolar therapy, which is the method of choice for release of inter-cranial pressure after brain trauma, may trigger the initial events that lead to FTD. Indeed, a strong as- sociation between brain trauma and FTD has been described in the past years by several groups, but no mechanism that could explain this association has been described to date. It is also known that hyperosmolarity can trigger the release of proinflammatory cytokines. Inflammation is a known risk factor for many neurodegenerative diseases.
Hock et al., (2018) Cell Reports 24, 987–1000
By Roland Fischer